1st May 2026
Choledochal Cysts: A Surgeon’s Guide to Diagnosis, Treatment and Long-Term Care
By Dr. Appou Tamijmarane | MS, FRCS (Edinburgh), FRCS (Glasgow)
Consultant General Surgeon specializing in HPB, Upper GI, and Advanced Laparoscopic Surgery
Fakeeh University Hospital, Dubai Silicon Oasis | DHA License No: 50530660-001
Published: May 2026 | Last reviewed: June 2026
Reading time: 14 minutes | This article is written for patients in Dubai who looking for information on choledochal cysts including the management and treatment options. Choledochal cysts are rare. With 35 years of surgical training specializing in HPB, including 18 years of biliary caseload in a regional cancer center in the NHS, I have encountered and operated on patients with this condition. That accumulated experience is what I bring to every consultation.
Key facts about choledochal cysts
- Congenital condition present from birth and is not caused by diet or lifestyle
- 85% of patients with choledochal cysts have no symptoms
- It is usually found incidentally on a scan when investigating other abdominal conditions
- Carries a small but cumulative lifetime risk of bile duct cancer if untreated
- The only effective treatment is complete surgical removal as no medication resolves it
- Outcomes after surgery are very good, with annual MRCP monitoring recommended
Quick answer for patients in a hurry
A choledochal cyst is a rare congenital condition where part of the bile duct balloons outward forming a localized dilatation. Around 85% of people have no symptoms and are diagnosed incidentally on a routine scan. The only curative treatment is complete surgical removal of the affected duct, followed by reconstruction of the bile drainage pathway. I have treated patients with this condition over 36 years of surgery, 19 of them as an NHS consultant in the UK and now at Fakeeh University Hospital in Dubai. The reassuring news is that outcomes are very good with timely treatment.
What is a choledochal cyst?
When patients first hear the term in my clinic, I usually start with this: a choledochal cyst is essentially a part of your bile duct that has “ballooned” out forming a localized dilatation in the tube that carries bile from your liver to your small intestine.
The cyst can develop anywhere along that duct system, from within the liver, down the length of the duct to where it joins the duodenum (the first part of the small intestine). Where exactly the dilatation sits is what defines the type of cyst, and this matters enormously for treatment, which I’ll come back to.
A few important facts to settle the anxiety this diagnosis often creates:
- It’s congenital. This means you were born with it. The cyst formed while you were a fetus, due to a combination of genetics and the way the tissues around your bile duct developed in the womb.
- It’s not your fault. I cannot stress this enough. Choledochal cysts are not caused by food, alcohol, smoking, stress, or any environmental factor. Just as everyone has a slightly different nose shape, everyone has small differences in the architecture of their internal organs. A choledochal cyst is one such variation.
- It’s rare. Choledochal cysts are uncommon worldwide, though they are reported more frequently in East Asian populations.
- Most people have no symptoms. Around 85% of patients I see with choledochal cysts feel perfectly well. The cyst is picked up incidentally, typically on an ultrasound or MRI ordered for an unrelated reason such as gallstones, a routine health check, or vague abdominal discomfort.
What are the symptoms of choledochal cysts?
This is one of the most common questions I’m asked, and the honest answer is that the symptoms, when they appear at all, can mimic many other, more common conditions. That’s why an experienced eye matters.
What is the Classic Triad?
In around 15% of patients, three symptoms appear together, for what we call the classic triad:
- Right upper abdominal pain
- Jaundice: a yellow tinge to the skin and the whites of the eyes
- A palpable mass in the right upper part of the abdomen
In the real world, very few adult patients present with all three together. That picture is much more common in children. In adult practice, by far the most frequent presenting symptom is persistent or intermittent pain in the right upper quadrant of the abdomen.
What I look out for that clinical experience has taught me
Right upper abdominal pain is most often caused by gallstones or indigestion. Most of the time, that diagnosis is correct. But some presentations don’t quite fit that pattern. When a patient’s symptoms feel inconsistent, I keep choledochal cyst on my differential. The clues I look for include:
- Recurrent pain that doesn’t behave like classical biliary colic
- Mildly abnormal liver enzymes with no clear explanation
- Fever and pain together, suggesting a bile duct infection (cholangitis)
- A history of unexplained pancreatitis
- A scan report mentioning “ductal dilatation” without a confirmed cause
When patients themselves often say the pain “doesn’t feel like normal indigestion,” they are usually right.
Why does early investigation matter?
The reason I push for full investigation rather than reassurance alone is that, untreated, choledochal cysts can lead to:
- Cholangitis: repeated bile duct infections
- Pancreatitis: inflammation of the pancreas
- Bile duct stones that block the duct
- Progressive liver damage over years
- Cholangiocarcinoma: bile duct cancer which is the most serious long-term concern
The cancer risk is small in any one year, but it accumulates over a lifetime. That’s why we don’t simply watch and wait, even when patients feel well.
A patient story that taught me a lasting lesson
Illness rarely arrives at a convenient time in your calendar. One patient I remember fondly came to me with jaundice stemming from a choledochal cyst complicated by multiple bile duct stones. The corrective surgery is major, even in a fit patient it carries a small risk of death. She was breastfeeding her six-month-old baby and wanted to continue until her child was two years old. Having the surgery could risk her continuing, so after a long and careful conversation, the patient chose to delay the surgery. We managed her symptoms and her bile duct stones through her acute crisis and she continued breastfeeding, living happily with her family.
That case highlights that the right time for surgery is rarely just a clinical question, it is a life question. Factoring clinical management and patient life choices for successful outcomes only happens with strong patient-doctor relationships are built on trust and understanding.
How is a choledochal cyst diagnosed?
In my own clinic, the diagnostic pathway is structured and methodical. Here’s exactly how I work through it.
Step 1 Blood tests
I start with liver function tests and inflammatory markers. If the liver enzymes (ALT, AST, ALP, GGT, bilirubin) are outside the normal range, that justifies further imaging.
Step 2 Ultrasound scan
Ultrasound is the first-line imaging investigation. It’s quick, safe, involves no radiation, and is excellent at identifying bile duct dilatation. If the ultrasound suggests a cyst or any abnormality of the duct, we move on to more detailed imaging.
Step 3 MRCP (Magnetic Resonance Cholangiopancreatography)
MRCP (Magnetic Resonance Cholangiopancreatography) is the investigation of choice for choledochal cysts. It is a specialized MRI that maps the liver, gallbladder, bile ducts, and pancreas in fine detail. The scan tells us where the cyst sits, how large it is, whether other parts of the biliary tree are affected, and whether stones are present. Crucially, it is non-invasive and involves no radiation.
Step 4 CT scan (when needed)
If imaging raises concern about a mass or possible cancer within or alongside the cyst, a CT scan gives us a highly detailed picture of the surrounding structures and helps with surgical planning.
Step 5 ERCP (only when therapeutic intervention is needed)
ERCP or Endoscopic Retrograde Cholangiopancreatography, combines an endoscopic camera passed through the mouth with X-ray imaging. It’s an invasive procedure, so I reserve it for situations where I need to do something, typically remove stones from the duct, place a stent, or take a tissue sample. In the modern diagnostic pathway, MRCP has largely replaced ERCP as a purely diagnostic test.
The Todani classification explained for patients
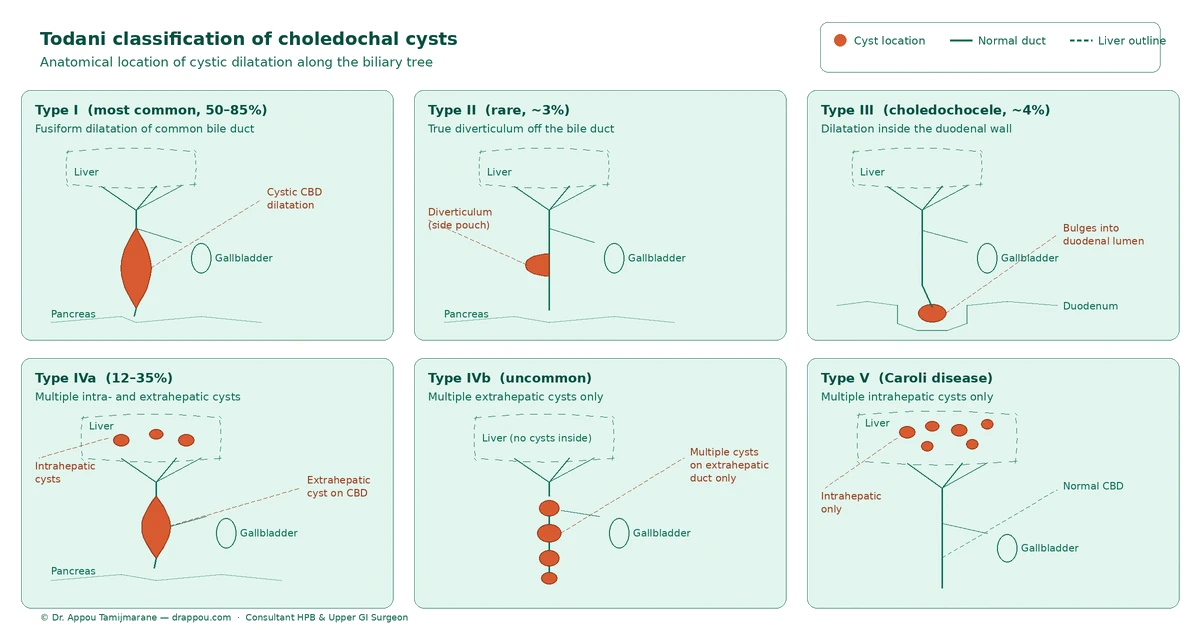
When you read your scan report, you will probably see a phrase like “Type I choledochal cyst on the Todani classification.” This may sound intimidating, but the idea is simple. Todani is a system that names the cyst based on where in the biliary tree it sits. That location, in turn, dictates the surgical approach.
Here’s the simplest way I explain it to my patients:
- Type I: A cyst on the bile duct outside the liver. This is by far the most common form, accounting for 50–80% of all choledochal cysts.
- Type II: A small “side pouch” off the bile duct, like a diverticulum. Rare (around 3%).
- Type III: A cyst at the very end of the bile duct, where it pokes into the wall of the duodenum (called a choledochocele). Around 4% of cases.
- Type IV: Multiple cysts. Type IVa involves cysts both inside and outside the liver. Type IVb involves multiple cysts outside the liver only. Together, Type IV accounts for around 12–35% of cases, the second most common pattern.
- Type V: Multiple cysts confined to the bile ducts inside the liver. This is also known as Caroli disease.
The diagram below shows each of these types along the biliary tree at a glance.
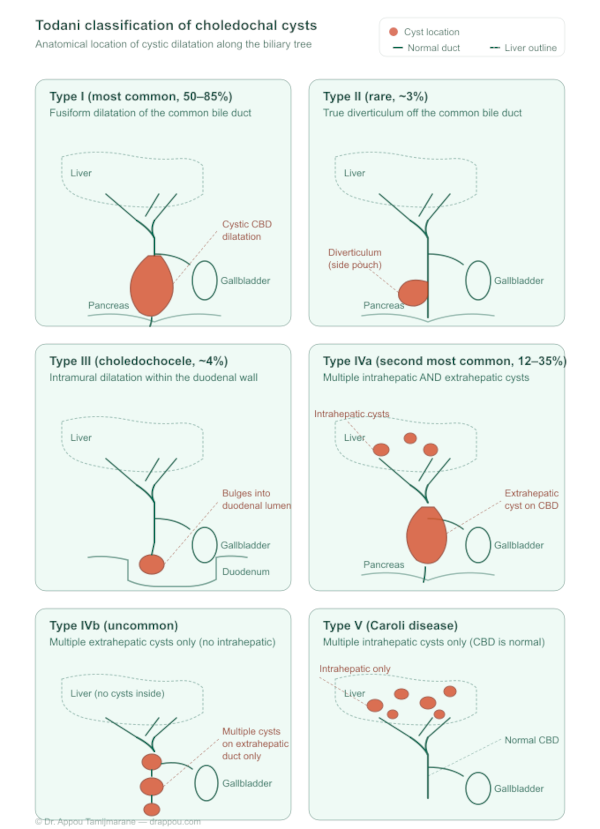
The reason this classification matters is that the surgical plan changes significantly between types. Type I and Type IV are the two most common adult presentations and are managed with complete cyst excision and biliary reconstruction. Type II is a simpler diverticulectomy. Usually endoscopic management is used for Type III and Type V (Caroli disease) may need a partial liver resection or, in advanced bilateral disease, consideration of a liver transplant.
Why is the whole duct removed?
Many patients ask me, “If my cyst is small and I have no symptoms, why operate at all?” It’s a fair question and I want to answer it directly.
There is no medical treatment for a choledochal cyst. No tablet, diet, or lifestyle change will make it go away. Drainage alone, or partial removal, leaves residual abnormal tissue behind and abnormal bile duct tissue is the tissue that, over years, can develop into cancer.
The aim of the operation is therefore twofold:
- Remove the abnormal duct entirely: including the cyst, the gallbladder, and any affected portion of the duct, ideally as a single, intact piece.
- Reconstruct the bile flow so bile can drain freely from the liver into the intestine again.
The Roux-en-Y hepaticojejunostomy
The gold-standard reconstruction is called a Roux-en-Y hepaticojejunostomy. The name sounds complicated; the principle is elegant.
We remove the entire affected bile duct in one intact piece which prevents bile or stones from spilling into the abdomen during surgery. Then we take a loop of small bowel and directly connect it to the healthy duct opening at the liver. The result is a clean, stone-free pathway for bile to drain from your liver into your intestine. That pathway is also far more resistant to future cancer development than the original abnormal tissue.
Two specific reasons I prefer this reconstruction:
- Oncological safety by removing the entire abnormal duct, we substantially reduce (though never eliminate) the long-term cancer risk.
- Mechanical longevity the Roux-en-Y configuration discourages food contents from refluxing back up into the bile duct, which reduces the risk of recurrent infections.
My surgical training in liver and biliary work spans institutions including the Royal Free Hospital London, Queen Elizabeth Hospital, Birmingham, and the Royal Infirmary of Edinburgh — culminating in a Norman Tanner Medal from the Royal Society of Medicine for work on hepatic surgery technique.
For Type V (Caroli) disease, where the cysts are entirely within the liver, treatment may require
liver resection of the affected portion. In severe, diffuse cases,
liver transplantation is considered.
Open, laparoscopic, or robotic surgery, which approach is right?
Patients often ask whether their cyst can be removed through “keyhole” surgery. The honest, surgeon-to-patient answer is this:
A complete cyst excision requires very careful dissection of the bile duct away from the major blood vessels behind it (the portal vein and hepatic artery), as well as careful handling of the pancreas where the lower end of the duct sits. The plane of dissection has to be perfect, being too aggressive risks injuring blood vessels or too cautious risks leaving abnormal tissue behind.
For this reason, open surgery still gives the surgeon optimal views and access for the most reliable, safest, and complete excision in adult patients. In carefully selected patients, typically those with simpler Type I anatomy, no previous inflammation, and no concern about cancer, minimally invasive approaches are becoming a credible option. As technology continues to advance and surgeon experience grows, I expect robotic options to increase.
The bottom line: the
best operation is the one that removes all the abnormal tissue safely. That is what I will plan for you, and we will discuss the trade-offs of each approach openly before any decision is made.
What about recovery, follow-up, and long-term cancer risk?
After surgery, you’ll typically spend a few days in hospital. Recovery from open Roux-en-Y reconstruction is usually 6–8 weeks back to normal activity, with most patients eating and walking comfortably within the first week.
Why we follow you up for life
Even with the most meticulous excision, a small portion of the bile duct usually has to be left behind at the lower end where the duct meets the pancreas, and at the top end where the duct enters the liver. Both of those segments retain a small, residual long-term cancer risk. For this reason, I personally recommend annual MRCP imaging after this surgery, indefinitely. This is a non-invasive scan, and it allows us to detect any change at the earliest possible stage. Most of my post-operative patients live entirely normal lives between these annual scans.
Symptoms to watch for after surgery
Please attend an emergency department urgently if, at any point after your surgery, you develop:
- New jaundice yellowing of the skin or eyes
- Fever with abdominal pain possible cholangitis
- Persistent vomiting or inability to keep food down
- Significant unexplained weight loss
- A return of the pain pattern that originally led to your diagnosis
These symptoms don’t always mean something serious, but they always deserve to be checked.
When should you see a specialist?
You should ask for an HPB (hepatobiliary) surgical opinion if:
- A scan has reported “bile duct dilatation” or “possible choledochal cyst”
- You have had recurrent right upper abdominal pain that has never been fully explained
- You have unexplained jaundice or repeatedly abnormal liver function tests
- You have had unexplained pancreatitis, particularly more than once
- You have a known choledochal cyst and you have not had recent surveillance imaging
You can also read my related guides on
liver cysts and
malignant liver tumors for context on related biliary conditions.
A final word
If you have just been told you have a choledochal cyst, I want to leave you with this. It is a rare condition, but it is a known condition with a clearly defined treatment pathway and very good long-term outcomes when managed by an experienced HPB surgeon. The diagnosis can be unsettling, especially when you read about cancer risk, but the entire purpose of the surgery I have described is precisely to address that risk proactively, before it becomes a problem.
Take your time. Ask questions. Bring a family member to your consultation. And get a second opinion if it gives you peace of mind, I encourage that for every patient considering major surgery.
Book a consultation with Dr. Appou Tamijmarane
Fakeeh University Hospital, Dubai Silicon Oasis
+971 503 567 569 (tel:+971503567569)
info@drappou.com
Chat on WhatsApp
Book an appointment online
Further reading from trusted medical sources:
Frequently Asked Questions: Choledochal Cysts
1. What is a choledochal cyst?
A choledochal cyst is a rare congenital condition where part of the bile duct balloons outward, forming a localized dilatation in the tube that carries bile from the liver to the small intestine. It develops before birth due to genetics, not diet, alcohol, or lifestyle. Around 85% of people with a choledochal cyst have no symptoms and are diagnosed incidentally on a scan done for an unrelated reason.
2. What are the symptoms of a choledochal cyst in adults?
In adults, the most common symptom is intermittent or persistent pain in the right upper abdomen. Around 15% of patients present with the classic triad: right upper quadrant pain, jaundice (yellowing of the skin or eyes), and a palpable abdominal mass. Other warning signs include unexplained pancreatitis, recurrent fever with abdominal pain, and persistently abnormal liver function tests. Around 85% of adults have no symptoms at all and are diagnosed incidentally on a scan.
3. Can a choledochal cyst become cancerous?
Yes, an untreated choledochal cyst carries a small but cumulative lifetime risk of developing into cholangiocarcinoma (bile duct cancer). This risk does not disappear on its own, it accumulates over years, which is why complete surgical removal is recommended even in patients with no symptoms. After surgery, a small residual risk remains at the duct margins, which is why annual MRCP surveillance is recommended indefinitely.
4. Is surgery always necessary for a choledochal cyst?
Yes. There is no medication, diet, or non-surgical treatment that will resolve a choledochal cyst. Partial removal or drainage alone leaves abnormal tissue behind, which retains a cumulative cancer risk. The only curative treatment is complete excision of the affected bile duct, followed by Roux-en-Y hepaticojejunostomy reconstruction to restore bile drainage from the liver to the intestine.
5. What is the Todani classification of choledochal cysts?
The Todani classification categorizes choledochal cysts by their location in the biliary tree. Type I (50-80% of cases) is a dilatation of the common bile duct outside the liver and is the most common. Type II is a rare side diverticulum (~3%). Type III is a choledochocele at the duct’s lower end (~4%). Type IV involves multiple cysts both inside and outside the liver (12-35%). Type V (Caroli disease) affects only the intrahepatic ducts. The type determines the surgical approach.
6. What is a Roux-en-Y hepaticojejunostomy and why is it used for choledochal cysts?
A Roux-en-Y hepaticojejunostomy is the gold-standard reconstruction performed after choledochal cyst removal. Once the abnormal bile duct is completely excised, a loop of small bowel is connected directly to the healthy duct opening at the liver. This creates a clean, cancer-resistant pathway for bile to drain from the liver into the intestine. The configuration also prevents food contents from refluxing back into the bile duct, reducing the risk of recurrent infections.
7. How is a choledochal cyst diagnosed?
Diagnosis follows a stepwise pathway. Blood tests (liver function tests) come first. If abnormal, ultrasound is the first-line imaging investigation. When ultrasound suggests bile duct dilatation, MRCP (Magnetic Resonance Cholangiopancreatography) is the investigation of choice as it maps the entire biliary tree in detail without radiation. A CT scan is added if cancer is suspected. ERCP is reserved for therapeutic intervention only, not routine diagnosis.
8. What is the recovery time after choledochal cyst surgery in Dubai?
After open Roux-en-Y reconstruction, most patients spend 3-5 days in hospital and return to normal activity within 6-8 weeks. Most patients are eating and walking comfortably within the first week. Annual MRCP imaging is recommended indefinitely after surgery to monitor the small residual risk at the duct margins. Choledochal cyst surgery is performed at Fakeeh University Hospital in Dubai Silicon Oasis by Dr. Appou Tamijmarane, a consultant HPB surgeon with 35 years of biliary surgical experience.
9. Can a choledochal cyst be treated with keyhole (laparoscopic) surgery?
In selected patients, typically those with simpler Type I anatomy, no previous inflammation, and with no concern about cancer, minimally invasive approaches are a credible option. However, complete cyst excision requires very careful dissection near major blood vessels (the portal vein and hepatic artery), and open surgery still provides the most reliable access for safe, complete removal in adult patients. The best operation is the one that removes all abnormal tissue safely, and the approach is discussed individually with each patient.
10. Where can I get choledochal cyst surgery in Dubai?
Choledochal cyst surgery in Dubai is performed by Dr. Appou Tamijmarane at Fakeeh University Hospital, Dubai Silicon Oasis. Dr. Tamijmarane is a consultant HPB (hepato-pancreato-biliary) and Consultant General Surgeon with 35 years of surgical experience, including 18 years managing biliary caseload at a regional cancer center in the NHS UK. He holds the FRCS (Edinburgh) and FRCS (Glasgow) and is licensed by the Dubai Health Authority (DHA License No: 50530660-001). Consultations can be booked at +971 503 567 569 or via the
hospital online booking system.
Medical disclaimer: This article is for general educational purposes and is not a substitute for individual medical advice, diagnosis, or treatment. If you are concerned about your symptoms or your diagnosis, please consult a qualified healthcare professional. Dr. Appou Tamijmarane is licensed by the Dubai Health Authority and practices at Fakeeh University Hospital, Dubai Silicon Oasis.